A Vagina Explained in Full
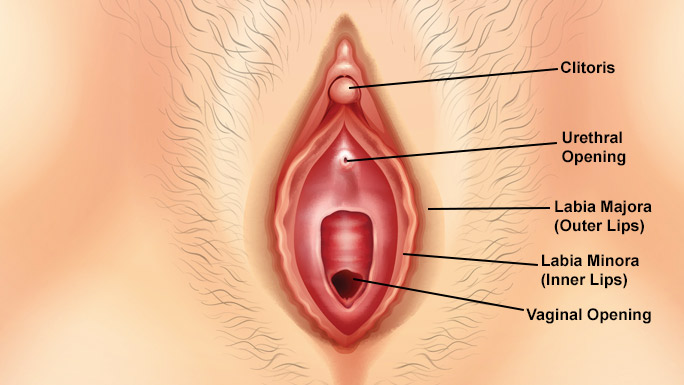
Vulva is the external genital organs of the female, including the labia majora, labia minora, clitoris, and vestibule of the vagina. (In common speech, the term "vagina" is often used improperly to refer to the vulva or female genitals generally, even though strictly speaking the vagina is a specific internal structure and the vulva is the exterior genitalia only. Calling the vulva the vagina is akin to calling the mouth the throat.)
The vulva is the opening to the reproductive system. Its functions are the passage of urine, the opening for mating and the birth canal. Included in the vulva's structure are the lips, vestibule and clitoris. The vulva lips are located at the opening and appear wrinkled and dry when the cow is not in heat. A secondary sign of heat, however, is when the vulva swells and appears moist and red.
The soft mound at the front of the vulva is the mons pubis, or specifically for humans, the mons veneris or "mount of Venus". After puberty it is covered with pubic hair to some extent, the amount being determined primarily by heredity. The labia majora or large lips extend on either side of the vulva, and may also be covered with pubic hair. The labia majora entirely or partially hides the other parts of the vulva. The colour of the outside skin of the labia majora is usually close to the overall skin colour of the individual, although there is considerable variation. The inside skin is often pink or brownish.
Labia majora
Two large lips of folded skin extend from the mons pubis downwards and backwards to fuse in the perineum about 2 cm anterior to the anus. The smooth skin contains fatty tissue and sebaceous sweat glands which are responsible for the sexual scent. When a girl has not yet reached puberty her labia majora are covered by pigmented skin, meaning that it will have a colour in the labia, it also contains sebaceous glands, these glands are oil-secreting. After puberty, her labia majora will be covered by coarse hair, depending on heredity the pubic hair may be abundant or scarce, with the inner sides being smooth and hairless and having sweet glands.
Labia Minora
Two thin lips pendulous folds of pigmented skin, are homologues of the ventral surface of the penis and are not usually visible unless the labia majora are parted or in the aroused state.
Labia minora is the flaps of delicate flesh that meet the hood of the clitoris at the front of your vulva and run down either side of the vaginal opening. They are nestled between the labia majora which protects them. Size and colour vary enormously from woman to woman. Some have labia that hang down five or more centimetres from between their labia majora, others have labia minora that are tiny and are little more than creases between the inside surface of their labia majora and their vulva. Colour is not just race related. Women can have labia in any shade from light pink to dark brown.
Every woman's vulva (or external genitalia) looks different. The labia majora (or outer lips) can be large or small or short or long. And the labia minora (inner lips) can similarly be large or small or short or long, full or thin, etc. The inner lips can also vary in texture and colour, with some women having pink lips and some women having brownish/black, and others having everything in between. This variation is what makes us all unique! What you describe (that your labia minora stick out of your labia majora) is perfectly normal and common.
Clitoris
Clitoris is a female erogenous organ capable of erection under sexual stimulation. A female homologue of the male penis, the clitoris develops (as does the penis) from the genital tubercle of the fetus, and it plays an important role in female sexual response. There is no standard size or shape for the hood. Some women have large clitoral hoods that completely cover the tip of the clitoris. Some of these can be retracted to expose the clitoral head, others do not retract. Other girls have smaller hoods that do not cover the full length of the clitoris, leaving the head exposed all the time.
Most women achieve orgasm through the friction of the clitoris against the man's pubic bone while engaged in intercourse or through stimulation of the clitoris by manual or oral contact. The clitoris is a shaft of enforceable tissue, built just like a small penis, with a sexually sensitive head (the glans) at its tip, just like the head of a small penis. It comes equipped with a foreskin or prepuce, just like an uncircumcised penis, and during sexual excitement, the foreskin retracts, exposing the glans of the clitoris, the little "button" most people think is the entire organ. Unlike the shaft of the penis, which is free-hanging, the shaft of the clitoris lays vertically along the body's midline, covered and never seen, just beneath a layer of fat and skin. The shaft of the clitoris reaches down toward the vagina and then splits to each side.
The visible glans of the clitoris, which is hooded by a prepuce formed by the meeting of the labia minora, is, however, only the outward and visible manifestation of much more extensive structures of erectile tissue, which form a padding over the pubic bone. These concealed parts are anatomically continuous and functionally linked to the vagina. The whole structure is densely packed with nerve endings: although there is a similar number to those of the penis, they are much more concentrated and closer together. It may be noted that although anatomically speaking, the clitoris is homologous to the penis, the female genitalia is far more differentiated than those of the male: instead of one organ which conveys sperm, and urine and is the source of sexual pleasure, a woman has three different parts for these distinct purposes. When erotically stimulated the clitoris becomes engorged and erectile; when a high degree of arousal is reached it retracts, with the effect that it appears to have reduced in size. Vaginal lubrication takes place along with the engorgement of the outer part of the vagina. When sexual excitement reaches its peak orgasm takes place with rhythmic contractions of the clitoris and vagina. Unlike men, women have the capacity for multiple orgasms without an intervening refractory period.
In intercourse, if the partners are well-adjusted in terms of size and posture, the woman will position herself so that her clitoris is placed between her symphysis and her partner's. This is called "clitoris seizure." Then, at the end of each inward stroke he makes, she will give a little downward and outward roll of the pelvis which presses her clitoris rather firmly between the two bones and rubs it upward. This is called "clitoral excursion."
When the clitoris becomes stimulated during intercourse, it gradually recedes into the prepuce of the clitoris. Regardless of sexual position or intensity of caressing, it becomes difficult to stimulate the clitoris directly. Sometimes men are unable to locate the clitoris during intercourse. Some women who prefer stimulation of the clitoris try to delay the insertion of the penis. It is difficult to stimulate the clitoris with the forward movement of the penis, but it can move back and forth somewhat from pressure on the labium minor. When the penis is inserted deeply and rotated, the movement applied to the labium minor is transmitted to the epidermis, indirectly stimulating the clitoris. Some claim that close and strong contact between pubic bones applies pressure to the clitoris and gives the woman pleasure, but this is not always true.
Although the clitoris is such a small and apparently insignificant organ, there are and have been widespread conceptions that it is dangerous and threatening. There are substantial areas of the world today, in Africa and the Middle East, in which clitoridectomy is still routinely practised on ritual and hygienic grounds*, though the number of cultures that practice it is far fewer than those in which some kind of circumcision of the penis is performed on boy children or youths in transition to manhood. The practice is deeply embedded in national and religious cultures and has proved very difficult to extirpate attempts to do so having caused crises for colonial powers in Africa. While many of the cultures which practice it are Islamic, clitoridectomy is not coterminous with the Muslim world, being found among other religious groups in the regions in which it is common, and not being practised in all Islamic nations.
Vagina
The vagina is the opening that is located directly below the urethral opening (where you pee from). The opening is called an orifice, as are other openings in your body. The vagina is a muscular, highly expandable, tubular cavity leading from the vestibule to the uterus. The vagina is the structure penetrated during vaginal intercourse, and it serves as an exit channel for menstrual flow. During vaginal intercourse, contact with this structure provides sexual pleasure in some women. The anterior vaginal wall is more densely innervated and more highly sensitive to stimulation than the posterior vaginal wall.
The average vaginal canal is three inches long, possibly four in women who have given birth. This may seem short in relation to the penis, but during sexual arousal, the cervix will lift upwards and the fornix may extend upwards into the body as long as necessary to receive the penis. After intercourse, the contraction of the vagina will allow the cervix to rest inside the fornix, which in its relaxed state is a bowl-shaped fitting perfect for the pooling of semen.
The size of the vaginal orifice varies inversely with that of the hymen. The orifice is capable of expansion during coitus and delivery. The ducts of the greater vestibular glands open on each side of the vaginal orifice, between it and the labia minora. With a decrease in oestrogen levels, the orifice becomes smaller. The vagina forms an angle of about 90 degrees from the uterus. The anterior wall is about 7.5 cm long and the posterior wall is about 9 cm long. In a nulliparous adult, the vagina is H-shaped in a section with transverse ridges or folds called vaginal rugae. The walls of the vagina are highly distensible. Part of the cervix protrudes into the vagina. The recess between the vaginal part of the cervix and the vaginal walls is termed the fornix.
The anterior fornix is the recess between the cervix and the anterior wall of the vagina and it is related to the bladder base and the fossa between the bladder and the uterus. The posterior fornix is the recess between the cervix and the posterior wall of the vagina. The posterior fornix is related to the recto-uterine pouch. It is deeper than the anterior fornix because of the angle that the cervix makes with the vagina. It is the site where semen collects after ejaculation. The lateral fornices are found between the lateral walls of the vagina and the cervix. Before puberty the rugae are absent. In the elderly, the vagina becomes narrower and less deep. The wall is less elastic and appears pale and smooth due to the loss of rugae.
G Spot
A rather high percentage of women do not reach the climax in sexual intercourse. For years, the clitoris was considered the only trigger for the female orgasm. The G-spot is a lump-like sensitive area felt through the upper vaginal wall, about halfway between the back of the pubic bone and the cervix, and was first discovered by German scientist Dr Ernst Grafenberg in the 1950s.
The G-spot has been identified as a sensitive area right behind the front wall of the vagina, between the back of the pubic bone and the cervix. (A man's "G-spot" is his prostate.) When this spot is stimulated during touching or sex, some women's orgasms are accompanied by "ejaculate" from the urethra. Ernst Grafenberg, who first wrote about female ejaculatory fluid in 1950, stated that fluid expelled by women during orgasm was not the urine, as was a common belief, but, instead, secretions that are similar to a man's ejaculate minus sperm.
Location Of The G Spot
The G-spot lies directly behind the pubic bone within the front wall of the vagina. It is usually located about halfway between the back of the pubic bone and the front of the cervix, along the course of the urethra and near the neck of the bladder, where it connects with the urethra. The size and exact location vary. Unlike the clitoris, which protrudes from the surrounding tissue, it lies deep within the vaginal wall, and firm pressure is often needed to contact the G spot in its unstimulated state. Usually, it is a lima-bean-sized, spongy area that responds to stimulation by hardening and swelling as blood rushes to it.
It is relatively difficult for a woman to explore the G-spot on her own because most do not have fingers long enough to reach it. Inserting an appropriate, safe, clean object into the vagina is probably required for self-exploration. Or working with a trusted partner can make for the enjoyable self-discovery of a woman's G-spot. Through experimentation, a woman can learn the type of stimulation that feels best to her. Penile stimulation is often more effective when done through steady and prolonged pressure, rather than with the usual penile thrusting, because the G-spot generally needs an intense and quite localized pressure.
Fallopian Tubes
Fallopian (felo-´pe-en), either of a pair of tubes extending from the uterus to the paired ovaries in the human female, also called oviducts, technically known as the uterine tube. At one end the long, slender fallopian tube opens into the uterus; the other end expands into a funnel shape near the ovary. The epithelium that lines the tube is covered with cilia that beat continuously toward the uterus. When an ovum is expelled into the peritoneal cavity from the ovary during ovulation, it is propelled into the wide-mouthed opening of the fallopian tube, through the tube, and into the uterus by the wavelike motion of the cilia.
If the ovum is fertilized, an event that normally takes place in the fallopian tube, and the embryo (fertilized ovum) implants in the tube, or another area outside the uterus, an ectopic pregnancy occurs. About 98% of ectopic implantations occur in the tubes, but other sites include the abdomen, ovary, and cervix. Immediate surgical removal of the products of conception is necessary to prevent hemorrhage and other complications resulting from ectopic pregnancy. The fallopian tubes are also the site of the most common surgical procedures used to prevent conception or cause infertility in women. Usually, the tubes are tied off in a procedure known as tubal ligation, although they are also sometimes excised or occluded by other methods.
Ovaries
Ovaries are small, oblong, pearl-coloured organs that lie just below the fallopian tubes on each side of the uterus. Ovaries produce ripe eggs about once a month, from about age 14 or 15 onward. As the egg develops each month, a nourishing fluid-filled sac forms around it, so that it is encapsulated or walled off from the rest of the ovary. This fluid-filled area, known as a cyst, is physiologically completely normal, a fact that many women don’t appreciate. At ovulation, when the egg is released and picked up by the fallopian tube, the cyst actually bursts as part of the ovulatory process, and the surrounding fluid is released into the pelvic cavity along with the egg.

After ovulation, in the space where the egg used to be, a second small cystic area known as the corpus luteum develops and begins to secrete progesterone. The corpus luteum eventually gets reabsorbed by the ovary. Frequently the process of egg development begins and a small cyst forms, but ovulation doesn’t occur at that particular site. In this case, a small cyst will be left in that area of the ovary for a while. Because of this monthly process of egg development and cyst formation, it is perfectly normal for a woman to have small fluid-filled ovarian cysts at almost any time throughout her reproductive life. In fact, ovaries nearly always have small cysts in them.
Whenever a woman gets a pelvic ultrasound for chronic pelvic pain, a fibroid, or for any other reason, her ovaries are also scanned and these cysts show. Small 1–3-cm cysts are usually normal because producing small physiological cysts that come and go is part of what normal ovaries do. They gestate little eggs, little cysts — or in energy medicine terms, young ideas ripe with potential.
Ovaries also produce hormones — including estrogen, progesterone and androgens — throughout the life cycle, though the amounts they produce change (not necessarily declining), depending upon a woman’s age. It has been commonly thought that ovaries become essentially nonfunctional after a woman stops having periods, but studies in healthy women have proven that ovaries maintain their ability to produce steroid hormones for several decades after menopause. (See Reference 1, link below.) Parts of the ovaries do start to decrease in size when a woman is in her thirties, and they do lose mass more rapidly after age 45 on average, but they are not the inert fibrous tissue masses they’ve been thought to be.
As women age, only the outermost covering (theca) of the ovary regresses, the part where the eggs grow and develop and where physiological (“functional”) cysts form. In midlife, the innermost part of the ovary (inner stroma) becomes quite active for the first time in our lives (see Reference 2, link below). Studies have shown that our ovaries can produce androgens, as well as progesterone and estradiol, long after menopause. These hormones are significant in preventing osteoporosis and also maintaining energy and libido. (See Reference 3, link below).
As women age, only the outermost covering (theca) of the ovary regresses, the part where the eggs grow and develop and where physiological (“functional”) cysts form. In midlife, the innermost part of the ovary (inner stroma) becomes quite active for the first time in our lives (see Reference 2, link below). Studies have shown that our ovaries can produce androgens, as well as progesterone and estradiol, long after menopause. These hormones are significant in preventing osteoporosis and also maintaining energy and libido.